James a RHD 9 year old boy was brought into ED after getting his right ring and middle finger caught in the car door. He has sustained a subungal haematoma of his ring finger and nail bed laceration of his middle finger. He otherwise has no medical and surgical history.
There are three main types nail bed injuries listed below.
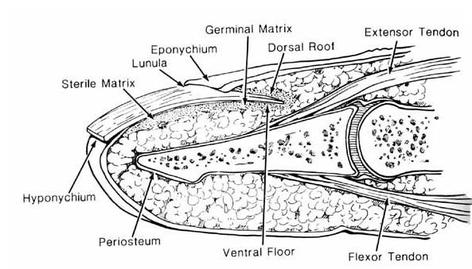
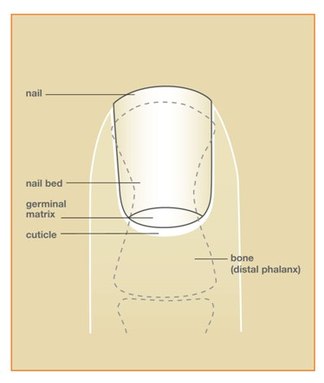
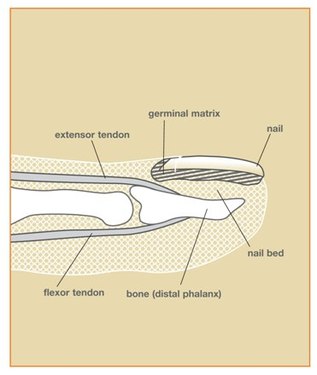
However, it is important to first understand the underlying anatomy. See images below.
There are three main types nail bed injuries listed below.
- Subungal Haematoma: bleeding beneath nail
- Nail Bed Laceration: laceration of the nail and underlying nail bed
- Nail Bed Avulsion: avulsion of nail and underlying nail bed
However, it is important to first understand the underlying anatomy. See images below.
Jones, T (2014)
 |  American Society for Surgery of the Hand (2006) |
It normally takes 3-6 months for nail to grow from the cuticle to the tip of the finger.
James' ringfinger has a haemtoma under the nail, see picture below, known as a subungal haematoma.
James' ringfinger has a haemtoma under the nail, see picture below, known as a subungal haematoma.

Jones, T (2014)
| When and how would you decide to treat a subungal haematoma? When it is painful or covers >50% of the nail (Jones, T, 2014). However, this is controversial. The subungal haematoma is evacuated using trephination. There are different methods of haematoma evacution, with the same goal; to create a small hole to allow blood evacuation and relieve pressure, thus improving pain. This can be done with a sterile needle, an 18 gauge needle (inserted, twirling into the nail bed until dark blood evacuates, beware risk of injury to nail bed underneath), electric cautery (safest method as the hot tip cools when reaching haematoma, protecting the nail bed). NOTE: Trephination is contraindicated if the nail bed requires surgical repair | 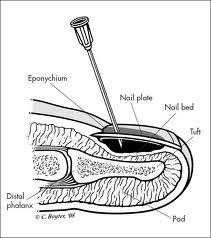 Jones, T (2014) |
Below is a photo of James' middle finger, demonstrating a nail bed laceration.

Jones, T (2014)
Normally the nail is intact and there is an underlying subungal haematoma covering >50% of the nail surface area. This is managed with tetanus, antibiotic prophylaxis and nail bed repair as described in detail below.
Nail bed avulsion injuries, as mentioned above are associated with nail and nail bed avulsion. If this is associated with significant loss of nail matrix this can be managed with nail bed matrix transfer from adjacent finger or second toe.
Nail bed avulsion injuries, as mentioned above are associated with nail and nail bed avulsion. If this is associated with significant loss of nail matrix this can be managed with nail bed matrix transfer from adjacent finger or second toe.
What associated injuries do you have to investigate for?
1. distal phalanx fractures or dislocations – common associated injury,
2. cuts of the nailbed and fingertip (pulp)
3. extensor of flexor tendon laceration
4. digital nerve laceration
Xrays were taken of James’ right hand, of his middle finger, shown below, please describe:
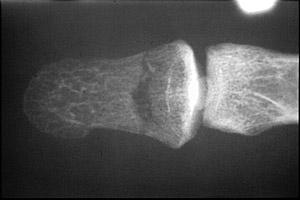
There is an extra-articular minimally displaced tranverse fracture of James' distal phalanx of his right middle finger. Distal phalangeal fracture reduction and healing is important to final nail formation. Poor reduction will result in irregularities of the nailbed. However, lateral views would need to be obtained to ensure no displacement of the fracture. Fixation will depend on the fracture.
What are the basic principles of nail bed repair?
Nail bed repair
What are the basic principles of nail bed repair?
- Minimal debridement
- Preservation of as much tissue as possible
- Atraumatic wound care
- Splinting with the nail
Nail bed repair
- Always give antibiotics and tetanus
- A digital block of 1% lidocaine hydrochloride without adrenaline (Children may require procedural sedation and analgesia)
- The hand should be prepared with povidone-iodine (Betadine) and covered with sterile drapes.
- Exsanguinate the injured finger, in a distal to proximal direction, a tourniquet will provide a blood-free field
- The nail is elevated using the blades of fine scissors, blunt dissecting technique should be used, the blades being placed under then nail bed until they reach the nail fold. Specific care is necessary to not injure the nail bed or nail fold.
- Once nail is separated from nail bed, it is gently removed and placed in Betadine
- Repair nailbed using 6-0 or smaller absorbable sutures. Ensure minimal debridement or tension on repair as this can result in scaring.
- Careful inspection of the nail is important. Only outer and dorsal surfaces of the nail should be cleaned, any nailbed fragments should be preserved for use as a graft. If tissue is not available and the defect is small enough, the area will heal effectively by secondary intention.
- The proximal nail should be reinserted into the nail fold. Why? - Keeps nail fold open for new nail growth - Protective cover for nail bed - Template for new nail to follow as it grows - Rigid split for any associated underlying fracture - Reduces postoperative discomfort and improves function
- Before replacement place a small hole in the nail, to allow drainage and thus prevent any developing haematoma that could separate the nail from the nailbed.
- The nail is then placed back in the nail fold as a stent and held in position by 5-0 or smaller nylon sutures or with adhesive, such as Dermabond. Nail fragments may be repaired together first with adhesive.
- If there is no nail available for splinting, alluminium or nonadherent guaze can be used.
- Dress the injured finger with nonadherent gauze and 2-inch gauze roll then splint the finger.
- Avulsion injury with nail bed matrix injury may require nail matrix transfer from adjacent injured finger or nail matrix transfer from second toe.
REFERENCES
Sutijono, D Mills, TJ (2015) Nailbed Injuries Treatment & Management. Accessed 4 Oct 2015. Available from: http://emedicine.medscape.com/article/827104-treatment
American Society for Surgery of the Hand (2006) Nail bed injuries, Chicago. Accessed 4 Oct 2015. Available from: http://www.assh.org/handcare/hand-arm-injuries/Nail-Bed-Injury#prettyPhoto
Jones, T. (2014) Nail Bed Injury. Orthobullets. Accessed 4 Oct 2015. Available from: http://www.orthobullets.com/hand/6109/nail-bed-injury
Sutijono, D Mills, TJ (2015) Nailbed Injuries Treatment & Management. Accessed 4 Oct 2015. Available from: http://emedicine.medscape.com/article/827104-treatment
American Society for Surgery of the Hand (2006) Nail bed injuries, Chicago. Accessed 4 Oct 2015. Available from: http://www.assh.org/handcare/hand-arm-injuries/Nail-Bed-Injury#prettyPhoto
Jones, T. (2014) Nail Bed Injury. Orthobullets. Accessed 4 Oct 2015. Available from: http://www.orthobullets.com/hand/6109/nail-bed-injury
 RSS Feed
RSS Feed
