Pathology
Benign or malignant orthopaedic tumours may involve the bones or soft tissues of the skeleton. Primary bone tumours are relatively uncommon but bony metastases are and will often be referred to orthopaedic surgeons for stabilisation. Pain (especially night pain), swelling and a change in size of a mass are worrying features that require further investigation.
Benign bone lesions on X-ray have well demarcated margins with no associated soft tissue mass or periosteal reaction. These include simple bone cysts, enchondromas, osteochondromas (exostoses) and aneurysmal bone cysts. Malignant lesions have an aggressive appearance on X-ray with bone destruction, poorly demarcated margins and periosteal reaction, often with an associated soft tissue mass. These include osteosarcoma and Ewing’s sarcoma.
Soft tissue tumours develop from the connective tissues other than bone, such as fat, muscle, tendon, nerve and blood vessels. Benign soft tissue lesions are usually present for many years in a superficial position and with no or minimal pain and no change in size. These include lipomas, haemangiomas and neurofibromas. Malignant soft tissue tumours are usually in a deep position, painful and increase in size rapidly. These include
liposarcoma, fibrosarcoma, leiomyosarcoma and synovial sarcoma.
After taking a full history and performing a thorough examination, investigations include:
Benign bone lesions on X-ray have well demarcated margins with no associated soft tissue mass or periosteal reaction. These include simple bone cysts, enchondromas, osteochondromas (exostoses) and aneurysmal bone cysts. Malignant lesions have an aggressive appearance on X-ray with bone destruction, poorly demarcated margins and periosteal reaction, often with an associated soft tissue mass. These include osteosarcoma and Ewing’s sarcoma.
Soft tissue tumours develop from the connective tissues other than bone, such as fat, muscle, tendon, nerve and blood vessels. Benign soft tissue lesions are usually present for many years in a superficial position and with no or minimal pain and no change in size. These include lipomas, haemangiomas and neurofibromas. Malignant soft tissue tumours are usually in a deep position, painful and increase in size rapidly. These include
liposarcoma, fibrosarcoma, leiomyosarcoma and synovial sarcoma.
After taking a full history and performing a thorough examination, investigations include:
- Blood tests (FBC, bone profile, U&E, protein electrophoresis, ESR, CRP)
- X-rays
- Further imaging (usually MRI)
- Image guided biopsy

Simple (unicameral) bone cyst of proximal femur. Note no cortical destruction, well defined borders and no soft tissue shadow (all features of benign pathology)
|
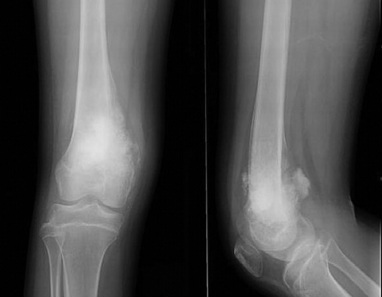
Osteosarcoma of distal femur in skeletally immature patient. X-rays show aggressive bone destruction, periosteal reaction, new bone fomration and soft-tissue enlargement (all features of skeletal malignancy)
|
If the biopsy of a lesion indicates malignancy, the patient requires staging, including investigation for metastases with a CT chest (most common site is to the lung) and bone scan. Surgical excision is performed with concurrent chemotherapy and radiotherapy as guided by oncologists.
Simple bone cyst
Found in the growing skeleton, often in the proximal humerus and femur. They are usually asymptomatic until a fracture occurs through the weakened cortical bone surrounding the cyst. A fracture usually stimulates healing of the cyst and apart from splinting in the form of
casts or braces, simple cysts rarely require further intervention.
Osteochondroma (exostosis)
A benign bone tumour which is often solitary but may be inherited with patients having many lesions in hereditary multiple exostoses. Pedunculated lesions arise from the joint line and grow away from the joint. May be left alone unless they cause local irritation or become symptomatic (pain may indicate malignant transformation which occurs in about 1%) in which case, they may be excised.
Osteosarcoma
Commonly seen in childhood and adolescence with a second peak in 6th decade. Most often affects distal and proximal femur, proximal tibia and proximal humerus. Histology reveals a high-grade spindle-cell tumour. Treatment is neo-adjuvant chemotherapy (pre- and post-surgery) with tumour excision and reconstruction with custom designed prostheses. If this involves the joint, this will be excised and replaced with a prosthesis.
Following treatment survival depends on whether the tumour had metastasised at presentation: 10 year survival 90% with no metastases but only 30% with metastases.
Ewing’s Sarcoma
Occurs in children and adolescents, most often in the femoral shaft. Patients receive neo-adjuvant chemotherapy followed by surgical excision and reconstruction. Survival rate at 5 years is 60-70% with no metastases, dropping to 20% when metastases are present.
Metastatic disease
Malignancies that have a predilection for spread to bone are lung, breast, prostate, kidney and thyroid. A primary bone tumour must be excluded in all cases. Treatment revolves around avoiding a pathological fracture. Risk is calculated using Mirel’s scoring system (increased risk with metastasis in the trochanteric region of hip, severe pain, lytic lesion on X-ray and involvement of >1/3 of bone cortex). Patients at high risk may undergo
prophylactic fixation of bones to prevent fracture (most commonly the femur will be stabilised with an intramedullary nail).
Soft tissue tumours
Require investigation if any part of the history or examination point towards malignancy (rapid increase in size, pain, deep lying tumour) with MRI and biopsy. If benign, marginal excision is adequate. Malignant soft tissue tumours require a wide margin of excision, following by radiotherapy to the tumour bed to reduce the recurrence rate.
Simple bone cyst
Found in the growing skeleton, often in the proximal humerus and femur. They are usually asymptomatic until a fracture occurs through the weakened cortical bone surrounding the cyst. A fracture usually stimulates healing of the cyst and apart from splinting in the form of
casts or braces, simple cysts rarely require further intervention.
Osteochondroma (exostosis)
A benign bone tumour which is often solitary but may be inherited with patients having many lesions in hereditary multiple exostoses. Pedunculated lesions arise from the joint line and grow away from the joint. May be left alone unless they cause local irritation or become symptomatic (pain may indicate malignant transformation which occurs in about 1%) in which case, they may be excised.
Osteosarcoma
Commonly seen in childhood and adolescence with a second peak in 6th decade. Most often affects distal and proximal femur, proximal tibia and proximal humerus. Histology reveals a high-grade spindle-cell tumour. Treatment is neo-adjuvant chemotherapy (pre- and post-surgery) with tumour excision and reconstruction with custom designed prostheses. If this involves the joint, this will be excised and replaced with a prosthesis.
Following treatment survival depends on whether the tumour had metastasised at presentation: 10 year survival 90% with no metastases but only 30% with metastases.
Ewing’s Sarcoma
Occurs in children and adolescents, most often in the femoral shaft. Patients receive neo-adjuvant chemotherapy followed by surgical excision and reconstruction. Survival rate at 5 years is 60-70% with no metastases, dropping to 20% when metastases are present.
Metastatic disease
Malignancies that have a predilection for spread to bone are lung, breast, prostate, kidney and thyroid. A primary bone tumour must be excluded in all cases. Treatment revolves around avoiding a pathological fracture. Risk is calculated using Mirel’s scoring system (increased risk with metastasis in the trochanteric region of hip, severe pain, lytic lesion on X-ray and involvement of >1/3 of bone cortex). Patients at high risk may undergo
prophylactic fixation of bones to prevent fracture (most commonly the femur will be stabilised with an intramedullary nail).
Soft tissue tumours
Require investigation if any part of the history or examination point towards malignancy (rapid increase in size, pain, deep lying tumour) with MRI and biopsy. If benign, marginal excision is adequate. Malignant soft tissue tumours require a wide margin of excision, following by radiotherapy to the tumour bed to reduce the recurrence rate.
