Assessment and management of fractures about the knee
by James Donaldson
Scenario: called to A&E to assess a 24 year old woman who fell off her horse and injured her knee.
History:
Age, occupation, sporting level and aspirations
Time/date of injury
Past medical/surgical history
Medication/drugs and allergies
Last ate/drank (for timing of emergency surgery if needed)
AP and lateral X-rays of the knee are required in all injuries
History:
Age, occupation, sporting level and aspirations
Time/date of injury
Past medical/surgical history
Medication/drugs and allergies
Last ate/drank (for timing of emergency surgery if needed)
AP and lateral X-rays of the knee are required in all injuries
- Often an MRI scan will be requested if there is a suggestion of ligament or meniscal injury (see soft tissue knee section)
- Bony injuries usually need surgery
|
Patella fracture
Mechanism: Direct trauma or eccentric quads contraction Signs & symptoms:
Management:
|

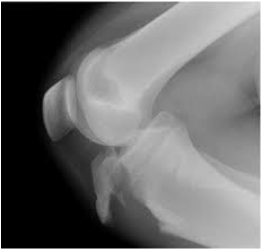
Lateral x-ray demonstrating displaced patella fracture
|
|
Distal femoral fracture
Mechanism: High energy (young) or low energy (elderly) Signs & symptoms:
Management:
|

AP & lateral x-rays of comminuted distal femur fracture
|
|
Tibial plateau fracture
Mechanism: Varus or valgus force with axial load Signs & symptoms:
|

AP x-ray demonstrating displaced, comminuted, intra-articular tibial plateau fracture
|
|
Tibial spine fracture
Mechanism: Similar to ACL injury. Associated with other intra-articular knee pathology in 40% of case. Signs & symptoms:
|

AP and lateral x-rays showing displaced tibial spine fracture
|
|
Tibial tuberosity fracture
Mechanism: Active quads extension with knee flexed. Signs & symptoms:
|
Lateral x-ray displaying displaced tibial tuberosity fracture
|
