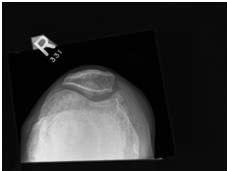
Another common one. A 62 year old male presents with worsening right knee pain and deformity. He underwent a knee injury in the 1980s but has managed to work and play sports on it up until recently. He has had a previous steroid injection with only very transient relief. Non-surgical management in the form of activity modification, analgesia, use of a walking aid and an off-loading brace have failed.
 |  |  |
What are the surgical options and their particular advantages / disadvantages?
This patient has fairly severe osteoarthritis with varus deformities of both knees.
Surgical options include:
High tibial osteotomy. Indications include:
- healthy patient in whom early failure of a TKR would be expected (less than 50 years old)
- non-obese and compliant with post-op rehabilitation
- predominantly one compartment involved
- no flexion contracture and good range of movement
A medial opening wedge or lateral closing wedge valgus osteotomy can be used to offload the diseased part of the joint. The patient needs to be non-weight bearing until the osteotomy has united which can be many weeks. The surgery alters the anatomy of the knee and can make a later knee replacement more difficult and less effective. A good outcome would be to maintain the knee for 8-12 years
Unicondylar Knee Replacement
Advantages compared to total knee replacement include:
- less blood loss, faster rehab and less morbidity
- smaller incision
- preserves the ACL and other knee compartments which may mean more normal knee kinematics
- compared to an osteotomy the rehabilitation is faster, it is easier to convert to a total knee replacement, has fewer short-term complications and should last longer.
Indications:
- controversial
- younger patients with normal lateral and patello-femoral compartments
- no fixed flexion deformity, intact ACL, varus <10 degrees, good range of motion
The down side is that the revision rate is much higher in the joint registries and conversion of a unicondylar knee replacement to total knee replacement is not universally as effective or predictable as a primary total knee replacement.
Total Knee Replacement
A total knee replacement is probably still the gold standard and would be my choice for the above patient. Predictable pain relief should be expected in the majority of patients and they can mobilise straight away. It is however designed for retirement level activities - which is why the above two options are attractive to some people.
Surgical options include:
High tibial osteotomy. Indications include:
- healthy patient in whom early failure of a TKR would be expected (less than 50 years old)
- non-obese and compliant with post-op rehabilitation
- predominantly one compartment involved
- no flexion contracture and good range of movement
A medial opening wedge or lateral closing wedge valgus osteotomy can be used to offload the diseased part of the joint. The patient needs to be non-weight bearing until the osteotomy has united which can be many weeks. The surgery alters the anatomy of the knee and can make a later knee replacement more difficult and less effective. A good outcome would be to maintain the knee for 8-12 years
Unicondylar Knee Replacement
Advantages compared to total knee replacement include:
- less blood loss, faster rehab and less morbidity
- smaller incision
- preserves the ACL and other knee compartments which may mean more normal knee kinematics
- compared to an osteotomy the rehabilitation is faster, it is easier to convert to a total knee replacement, has fewer short-term complications and should last longer.
Indications:
- controversial
- younger patients with normal lateral and patello-femoral compartments
- no fixed flexion deformity, intact ACL, varus <10 degrees, good range of motion
The down side is that the revision rate is much higher in the joint registries and conversion of a unicondylar knee replacement to total knee replacement is not universally as effective or predictable as a primary total knee replacement.
Total Knee Replacement
A total knee replacement is probably still the gold standard and would be my choice for the above patient. Predictable pain relief should be expected in the majority of patients and they can mobilise straight away. It is however designed for retirement level activities - which is why the above two options are attractive to some people.
 RSS Feed
RSS Feed
