This is a 73 year old lady who fell over onto her dominant outstretched left hand. Her radiographs are shown below:

What do you assess for when reviewing the radiographs of a Colles fracture?
What are the treatment options and what would influence your decision?
What are the treatment options and what would influence your decision?
Radiographic assessment should include:
- Fracture location, displacement and angulation
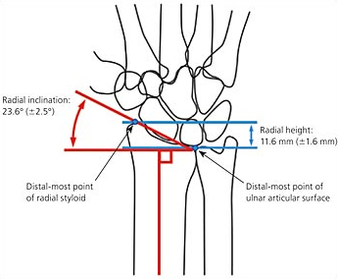
- Radial height. Normal = 11mm
- Radial inclination. Normal = 22 degrees
- Articular step off. The joint surface should be congruous.
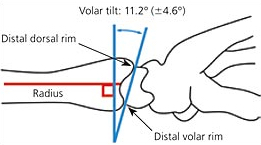
- Volar tilt. Normal = 11 degrees
- Fracture location, displacement and angulation
- Radial height. Normal = 11mm
- Radial inclination. Normal = 22 degrees
- Articular step off. The joint surface should be congruous.
- Volar tilt. Normal = 11 degrees
 |  |
Options are numerous and arguments can be made for each. There still remains little evidence of one modality over another.
1. A simple plaster of Paris can be used if the fracture is in an adequate position. This example is not and needs better reduction.
2. An attempt should always be made to reduce an acute fracture under a local block eg. haematoma block. A backslab should then be applied followed by a plaster of Paris at a later date.
3. Manipulation under anaesthesia is an option if the fracture is significantly displaced. It then needs to be held with a plaster of Paris. Often the distal fragment(s) are held in place onto the proximal bone with K-wires to prevent displacement. The wires can also be used to joystick the fragments back in to position. The wires are usually pulled out in clinic 4-6 weeks later.
4. Open reduction and internal fixation. Volar plating has become increasingly common. It allows accurate reduction of the fracture, rigid internal fixation and early mobilisation (AO principles). There are however higher risks with the surgery and metalwork.
5. External fixation is an option if the fracture is severely comminuted. It may be spanning (across the joint) or bridging (across the fracture only, which has the advantage of allowing joint mobilisation). Again K-wires can help augment the fixation.
1. A simple plaster of Paris can be used if the fracture is in an adequate position. This example is not and needs better reduction.
2. An attempt should always be made to reduce an acute fracture under a local block eg. haematoma block. A backslab should then be applied followed by a plaster of Paris at a later date.
3. Manipulation under anaesthesia is an option if the fracture is significantly displaced. It then needs to be held with a plaster of Paris. Often the distal fragment(s) are held in place onto the proximal bone with K-wires to prevent displacement. The wires can also be used to joystick the fragments back in to position. The wires are usually pulled out in clinic 4-6 weeks later.
4. Open reduction and internal fixation. Volar plating has become increasingly common. It allows accurate reduction of the fracture, rigid internal fixation and early mobilisation (AO principles). There are however higher risks with the surgery and metalwork.
5. External fixation is an option if the fracture is severely comminuted. It may be spanning (across the joint) or bridging (across the fracture only, which has the advantage of allowing joint mobilisation). Again K-wires can help augment the fixation.
 RSS Feed
RSS Feed
